Key Takeaways
- Hospitals and enterprises require structurally different AI architectures; retrofitting one for the other leads to systems that fail in real clinical use.
- HIPAA compliance is not a final checklist. It’s four core architectural requirements that must shape every data model and API from day one.
- Healthcare data breaches in 2023 affected over 133 million individuals, the highest on record,d making security a foundational design concern, not an afterthought.
- Healthcare organizations across California are among the fastest AI adopters in the U.S., driving strong demand for partners with genuine integration experience.
- The right development partner asks architecture-first questions upfront, not feature lists. No EHR and data governance discussion means they’re building in the wrong order.
Introduction
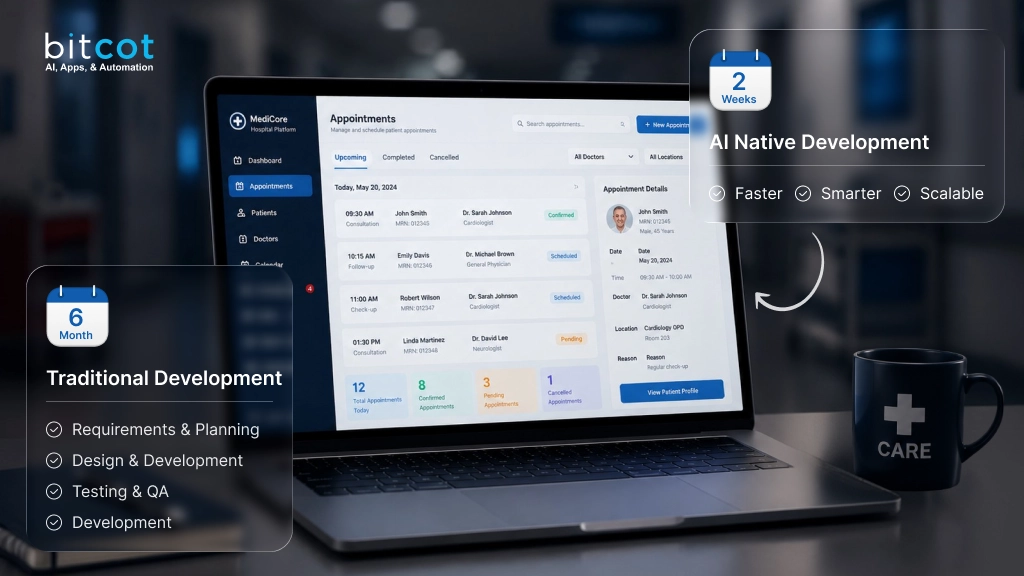
Most healthcare AI projects that fail do not fail because of weak AI models or poor user interfaces. They fail because the development team treated healthcare as a vertical specialization rather than as an architectural constraint. They built a capable AI application, added encryption, referenced HIPAA in the proposal, and delivered something that worked in the demo environment but broke down in the clinical one. The gap between those two environments, and why it consistently catches both vendors and buyers off guard, is what this guide is about.
According to the HHS Office for Civil Rights breach portal, healthcare data breaches in 2023 affected more than 133 million individuals, the highest single-year figure since the agency began tracking. That number reflects not just external attacks but a sustained pattern of applications that were built without the access controls, audit infrastructure, and AI-specific security layers that clinical environments require. The breach figure is a downstream measurement of upstream architecture decisions.
This guide addresses what separates a genuinely capable healthcare AI app development company from a general software shop with healthcare clients. It covers what HIPAA-guided practices require at the architecture level, the specific ways hospital and enterprise deployments differ, how to evaluate development partners based on process rather than portfolio, and what variables most reliably predict the scope of a healthcare AI engagement. California-based hospital systems and national enterprise health organizations will find the framework directly applicable to the vendor decisions they are making in 2026.
Why Hospitals and Enterprises Need Fundamentally Different AI App Architectures
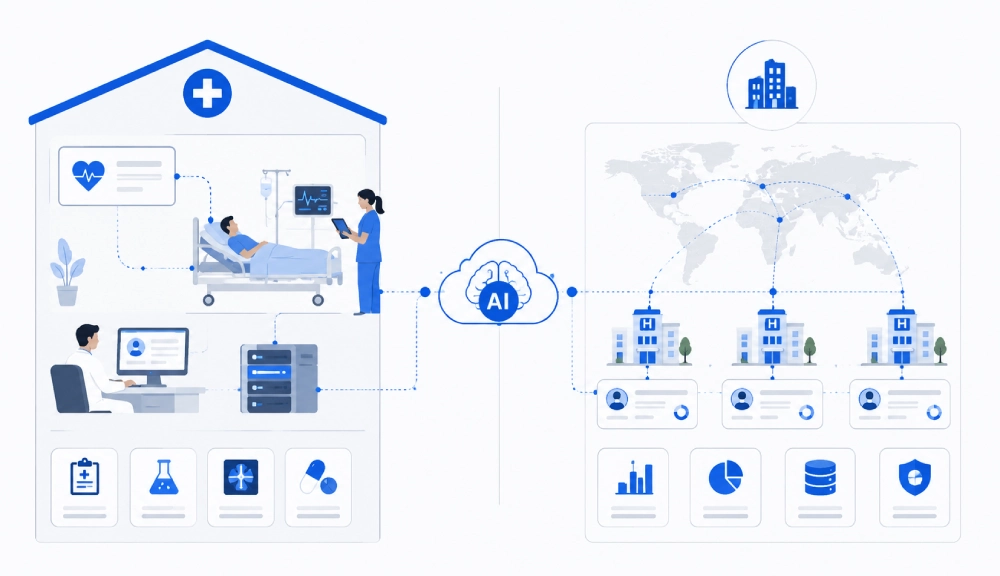
The most consequential decision any healthcare AI app development company makes happens before writing a line of code: determining whether the application is being built for a hospital environment or an enterprise health organization. These are not different points on the same spectrum. They have different data models, different integration requirements, different deployment constraints, and different failure modes. Development teams that use the same architecture template for both consistently produce the wrong result for at least one of them.
What Hospital AI Deployments Actually Require
Hospital environments require direct integration with electronic health record systems, clinical data repositories, and real-time patient monitoring infrastructure. The EHR integration layer is where the non-obvious complexity lives. Most development teams understand that hospital systems use HL7 FHIR APIs, but they underestimate what happens at the data normalization layer. Epic stores allergy records in a different schema than Cerner, which stores them differently from Meditech. A clinical AI feature that reads “active medications” from three hospital facilities that each use a different EHR platform is not making three identical API calls: it is reconciling three different data models into a common structure that the AI feature can reason over. In our experience building hospital-facing healthcare applications, this normalization work routinely consumes the largest share of integration development time, far more than the API connection itself.
Access control in a hospital environment is context-sensitive in ways that role-based control alone cannot capture. A hospitalist physician should assess all patients currently admitted to their unit, but not patients admitted to the orthopedics unit on the floor above. An on-call physician covering overnight should access active patients only, not historical records from the past six months. A clinical AI application that models access as “physician sees patient records” rather than modeling the actual context of the clinical relationship will either over-expose data or create workflow friction that causes clinical staff to route around the system. According to HealthIT.gov, over 96% of U.S. hospitals had adopted certified EHR technology by 2021, meaning the integration environment is mature, complex, and unforgiving of applications that model clinical access too simply.
Hospital deployments frequently require on-premises or hybrid deployment models. This is not primarily a preference: it reflects network isolation requirements that protect clinical systems from internet-facing threats, latency constraints for real-time clinical decision support tools, and legacy infrastructure that cannot be replaced on an application development timeline. A healthcare AI development company that builds exclusively for cloud-native SaaS deployment cannot serve this segment without forcing the hospital to change its infrastructure to fit the software, which is the wrong dependency direction for a clinical environment.

What Enterprise Healthcare AI Deployments Require
Healthcare enterprises, including multi-site health systems, payer organizations, and large medical device manufacturers, face a primary challenge that single-site hospital deployments do not: patient population variation across sites. An AI risk-stratification model trained on patient data from a single San Diego academic medical center will perform differently when deployed to a rural Sacramento community hospital or an underserved clinic in South Los Angeles. The patient demographic distribution, comorbidity patterns, and care-seeking behavior differ enough that a model optimized for one population produces less reliable outputs for another. Enterprise deployments that run a single shared model across all facilities without site-specific validation or calibration are operating a tool designed for one audience across multiple different ones.
Enterprise healthcare AI applications must be built API-first from the first sprint. The application will integrate with existing enterprise stacks: Salesforce for patient relationship management, Power BI or Tableau for operational analytics, and internal systems built years before the AI application existed. An AI/ML development partner that builds a monolithic healthcare application without an extensible, versioned API layer creates integration debt that compounds with every additional enterprise system that needs to connect. That debt is not just technical: it directly affects how quickly the clinical operations team can act on AI-generated insights, because the insights are trapped inside an application that does not speak to the systems where decisions are executed.
Multi-site data governance is the enterprise challenge that most development plans underestimate. An AI application deployed across 30 clinical sites in California and New York must maintain consistent access controls, audit logging, and data residency policies across all sites while allowing each site to operate within its local workflow constraints. The governance architecture for this, specifically who can authorize access changes at the site level versus the enterprise level, and how those decisions are audited, must be designed into the application before deployment, not negotiated after a policy conflict surfaces in production.
What HIPAA-Guided Practices Actually Require in Healthcare AI Architecture
HIPAA-guided practices in healthcare AI development are not a compliance layer added at the end of a project. There are four specific architectural requirements defined in the HIPAA Security Rule’s Technical Safeguards standard that must shape every technical decision from the data model forward. The important context that most development guides omit: the Security Rule was written before large language models existed. Applying it to AI healthcare applications requires interpreting requirements designed for human-created records against the behavior of systems that generate, infer, and transform data automatically.
Access Controls Mapped to Clinical Context
The Security Rule requires unique user identification, emergency access procedures, and automatic logoff. In a hospital AI application, unique identification means every API call touching patient data must carry an individually attributed, non-shared identity token. Sessions must time out based on inactivity thresholds calibrated to the clinical context: a 15-minute timeout appropriate for an administrative portal creates dangerous friction in an emergency department workflow. Emergency access pathways must be pre-built with their own audit trail, not improvised during an incident by granting temporary elevated permissions that are never revoked. A healthcare AI development company that implements team-level API keys or shared service accounts to simplify development is failing this requirement at its foundation, and the failure is invisible until a security review or incident makes it visible.
Audit Logging That Supports Post-Incident Investigation
The Security Rule’s audit controls requirement is not satisfied by standard application logging. The requirement is that logs must be usable for examining activity in information systems containing ePHI. For AI healthcare applications, this means every model inference request involving patient data must be logged with the input context, the output produced, the user identity, the timestamp, and the model version. Standard application logs stored in a mutable relational database do not meet this standard because they can be modified. Append-only storage with cryptographic integrity verification, such as AWS CloudTrail with CloudWatch Logs, Azure Immutable Blob Storage, or Google Cloud’s write-once buckets, produces tamper-evident records that remain useful for investigation even if an attacker gains application-level access.
Integrity Controls Reinterpreted for AI-Generated Clinical Content
The HIPAA integrity control requirement was designed for human-created records: to protect ePHI from improper alteration or destruction. Applied to AI healthcare applications, this requirement has a dimension that the original rule did not anticipate. When an AI model produces a clinical note summary, a risk score, or a treatment pathway recommendation that is recorded in a patient’s chart, the application must demonstrate what the model produced, when it produced it, which model version was running, and that the stored record has not been altered since generation. A clinical note that was AI-generated, then edited by a clinician, then stored under the AI attribution without a version history, creates both a patient safety risk and a records integrity exposure. Immutable write-once storage for AI-generated clinical content, with explicit human-review versioning, is the correct technical response to a requirement the original rule authors did not have to consider.
Transmission Security Across Networks You Do Not Control
Healthcare AI applications transmit patient data across networks that the development team cannot control: hospital Wi-Fi used by clinical tablets, consumer internet connections used by remote monitoring devices, and inter-facility VPNs with inconsistent security configurations. According to NIST SP 800-52 Rev. 2, TLS 1.3 is the current recommended standard for data in transit. Healthcare applications should not support TLS 1.0, 1.1, or SSL under any circumstances. For mobile healthcare applications, certificate pinning prevents interception attacks on untrusted networks by verifying not just that the server certificate is valid, but that it matches a specific expected value. This matters most for remote patient monitoring applications, where the mobile device is the patient’s own phone on their home Wi-Fi, not a managed enterprise device on a controlled hospital network.

How Do You Evaluate a Healthcare AI App Development Company in the USA?
Evaluating healthcare software vendors in the USA effectively requires looking past credentials and case study decks toward process signals. A vendor may have worked with healthcare clients for ten years and still approach your engagement with a general-purpose software development process that does not account for the architectural constraints that healthcare AI requires. The most reliable evaluation signals are revealed in how a vendor conducts the first technical conversation, not in what they have built before.
Threat Modeling as Architecture Input
The single most revealing question to ask a prospective healthcare AI development company: “Walk me through the threat modeling process you conduct before finalizing the architecture.” A vendor who responds by describing penetration testing, security scanning, or a compliance checklist is describing work that happens at the end of a project. Those are verification activities. A vendor who describes threat modeling as the process that produces the access control matrix, the API scoping decisions, and the audit logging architecture is describing threat modeling as an input to design, which is the correct relationship. The specific red flag to watch for: a vendor who says “we have extensive experience with HIPAA clients” but cannot describe what a Business Associate Agreement requires of their specific development workflow is relying on association, not demonstrated practice.
AI-Specific Security Literacy
General software security knowledge is not sufficient for healthcare AI development. Ask the vendor specifically about model inversion attacks, adversarial inputs to clinical prediction models, and prompt injection vulnerabilities in LLM-based features. If they cannot describe all three, they are not equipped to design secure AI features for a clinical environment. This is not esoteric knowledge: these are documented, actively exploited vulnerability classes that any development team shipping AI features into a healthcare environment must have addressed in their architecture before the first model is deployed.
Healthcare Integration Depth
Ask specifically about HL7 FHIR integration experience, and follow up by asking which EHR platforms they have integrated with and what the data normalization challenges were at each. FHIR R4 and SMART on FHIR are the current interoperability standards for clinical application integration in the U.S. According to the ONC 21st Century Cures Act Final Rule, health IT developers and providers are required to support standardized FHIR APIs. A vendor who cannot speak to the specific data normalization challenges across Epic, Cerner, and Meditech environments has not done this work at the depth that a production hospital integration requires.
Reference Deployments in Comparable Environments
Request case studies from deployments that match your environment in entity type and scale. A vendor with strong single-site hospital results may not have the architecture experience that a 30-site enterprise deployment requires. An enterprise software shop may produce over-engineered solutions for a community hospital that needs a focused, low-latency clinical tool. Ask specifically: “Have you deployed this type of application across multiple facilities with different EHR systems?” The answer reveals whether the vendor has encountered and solved the multi-site data normalization and governance challenges your engagement will require, or whether they will encounter them for the first time on your engagement.
Core Technical Stack: What Secure Healthcare AI Applications Are Built On
The technical stack for a production-grade healthcare AI application spans four layers, each carrying decisions that are difficult to change after deployment. Understanding what these layers require allows procurement teams to evaluate vendor proposals at the architecture level, not just the feature level.
Data Layer: Encrypted, Partitioned, and Privacy-Preserving for Training
Patient data at rest requires AES-256 encryption with managed key rotation. For AI model training, de-identification must go beyond field-level masking. Field masking removes obvious identifiers like name and date of birth, but it does not prevent re-identification when rare disease codes, unusual procedure combinations, or specific geographic data are present in the same record. Differential privacy adds mathematically verifiable noise to training datasets, making it provably difficult to reconstruct individual records from model outputs. For custom software development in healthcare, data partitioning by patient, facility, and data category must be defined in the schema design phase: retrofitting partition boundaries after patient data is already in production is operationally disruptive and technically expensive.
AI Model Layer: Validated Against Your Population, Not Just Held-Out Data
Healthcare AI models must be version-controlled with immutable deployment records. Every model deployed to a production clinical environment requires a documented validation dataset, performance benchmarks against defined clinical outcomes, and a rollback mechanism. The validation approach that most development teams get wrong: they validate on held-out data sampled from the same population used for training, then deploy to a clinical environment with a different patient demographic profile. A sepsis prediction model validated on academic medical center data performs measurably differently at a safety-net hospital serving a different patient population. Site-specific validation, or at minimum, site-specific performance monitoring with automated drift detection, is what production-grade clinical AI requires.
API Layer: Authenticated, Scoped, and Built for Integration
Every API endpoint exposing patient data or model inference must require individually-attributed authenticated requests with scoped tokens. Rate limiting on inference endpoints disrupts model inversion attack patterns, which require high query volumes to reconstruct training data. API versioning enables model and schema updates without breaking downstream integrations, a critical capability for enterprise healthcare environments with multiple consuming systems. A versioned, well-documented API is also the foundation for the digital transformation integrations that enterprise healthcare organizations need to connect AI outputs into operational workflows and analytics platforms.
Infrastructure Layer: Zero-Trust, Containerized, and Regionally Constrained
Healthcare AI infrastructure should use containerized Kubernetes deployments with network policies enforcing service-level isolation. Zero-trust architecture requires every service-to-service call to authenticate regardless of network origin, preventing lateral movement after an internal compromise. Infrastructure-as-code templates should be scanned for security misconfigurations in CI/CD pipelines before every deployment. Cloud environments should be configured with region-specific data residency constraints, particularly for applications serving California health systems subject to state privacy regulations that impose stricter data localization requirements than federal standards alone.
What Determines the Cost of Healthcare App Development with AI?
The scope of a healthcare AI development engagement is driven by a combination of variables that interact differently depending on the entity type and deployment environment. The most consistent pattern we observe across engagements: the security architecture workstream is the most persistently underestimated scope item in initial plans. Teams account for AI feature development and EHR integration but allocate insufficient scope to differential privacy implementation, audit log infrastructure, zero-trust configuration, and AI-specific input/output filtering. These are not optional additions: they are the foundational layer that all AI features sit on, and discovering their scope mid-engagement is what causes healthcare AI projects to run over plan.
AI Feature Complexity and Model Type
There is a fundamental difference in development scope between fine-tuning a pre-trained model (such as adapting a general-purpose LLM for clinical note summarization) and building a custom predictive model trained on an organization’s own patient population. Fine-tuned models reach initial deployment faster but require extensive output validation for clinical suitability, because the pre-training data includes non-clinical content that can surface as inappropriate outputs in a medical context. Custom models require curated training datasets, de-identification workflows, clinical outcome validation, and ongoing retraining infrastructure. The AI feature type is frequently the single largest scope driver in a healthcare AI engagement, and it must be defined precisely before any architecture work begins.
EHR and System Integration Depth
Integrating a healthcare AI application with an existing EHR, whether Epic, Cerner, Meditech, or an open platform like OpenEMR, requires navigating vendor-specific API constraints, authentication flows, and data model differences at the field level. The deeper the integration (read-write versus read-only, structured data versus clinical notes, real-time versus batch), the greater the development scope. Enterprise deployments integrating with multiple EHR platforms across different facilities are the most complex integration environments in healthcare technology, and the complexity is multiplicative, not additive: each additional EHR platform adds not just its own integration effort but the normalization layer required to reconcile its data model against the others.
Deployment Model and Infrastructure Scope
Cloud-native deployments on AWS, Azure, or Google Cloud Healthcare API carry a lower infrastructure setup scope because managed services handle underlying encryption, key rotation, and audit logging configuration. On-premises deployments for hospital environments with network isolation requirements carry a substantially higher infrastructure setup scope. Hybrid deployments that maintain patient data on-premises while running inference workloads in the cloud introduce additional complexity at the data synchronization, encryption key management, and network boundary layers. The deployment model should be determined by the clinical environment’s actual requirements, not by the development team’s infrastructure preferences. According to the U.S. Bureau of Labor Statistics, demand for developers in healthcare-adjacent roles is growing significantly faster than the overall software market, which affects both team availability and realistic timeline planning for healthcare AI engagements in 2026.
How to Hire a Healthcare AI App Development Company in the USA
Hiring a healthcare AI app development company is a procurement decision with consequences that extend well past the engagement itself. The architecture decisions made by the development team become the architecture your clinical operations team manages for years. Switching development partners mid-engagement in a healthcare AI project is significantly more disruptive than in most software categories, because the integration touchpoints, the data models, and the security architecture are all tightly coupled to the specific technical decisions the original team made.
Start the evaluation by defining your entity type, deployment environment, and EHR landscape precisely before issuing any RFP or proposal request. A hospital with three facilities all on Epic, has a different engagement profile than a 20-site enterprise health system on Epic, Cerner, and a custom legacy platform. Vendors who cannot ask questions that distinguish between these two environments in the first conversation are not operating at the level of specificity a healthcare AI engagement requires.
Request a technical discovery session before any scope or timeline discussion. Use it to evaluate the vendor’s question sequence: do they ask about data flows, integration points, access control requirements, and AI model risk before discussing features and timelines, or do they lead with capability demonstrations? Vendors who ask architecture-first questions in discovery sessions have built that discipline into their process. Vendors who lead with what they have built before are optimizing for familiarity rather than fit. The specific question that most reliably reveals process maturity: “What does your onboarding process look like for a new healthcare AI engagement?” Vendors who describe a structured architecture and security design phase with defined deliverables before development begins are describing the correct sequence. Vendors who describe it as starting with a kickoff and moving into sprints are describing a process designed for general software, not for healthcare.
For California-based hospital systems in San Diego or Sacramento, a development partner with direct experience in California’s state privacy regulations adds value beyond general U.S. healthcare knowledge. For enterprise health systems spanning multiple states, demonstrated experience with multi-state data residency management and enterprise integration at scale is the differentiating capability. Healthcare organizations in San Jose, Oakland, Irvine, and Long Beach should evaluate whether the vendor’s past engagements reflect the specific clinical complexity of their patient population and operational environment, not just the category of healthcare technology.
Our Perspective
The pattern we encounter most consistently when healthcare organizations come to us after a failed AI development engagement is predictable enough that we now ask about it directly in the first discovery call. The previous team built a capable AI application and then adapted it for healthcare use. They did not design for healthcare: they designed for software and then added healthcare constraints. That sequence always produces the same outcome: the access control model was designed for the demo environment, which had five user roles, not the production environment, which has 35 clinical role variants with context-specific permissions. The model was validated on held-out data from the training population but never tested against the actual patient demographics at the deployment site. The audit log worked correctly in single-facility staging but broke under the query load of a multi-facility enterprise deployment.
At Bitcot, we have built healthcare applications for organizations across San Diego, Los Angeles, and New York, spanning hospital-facing clinical tools and enterprise administrative platforms. The consistent pattern in engagements that succeed: security architecture and data governance decisions are made in the design phase, before features are scoped. When the access control matrix is defined before the user interface, the UI gets built to reflect clinical reality rather than demo convenience. When the audit logging architecture is defined before the database schema, the schema includes the partition boundaries and record identifiers that the audit system requires. These are not process preferences: they are the sequencing decisions that determine whether a healthcare AI application operates reliably in production or requires partial rebuilding six months after launch.
The organizations that build healthcare AI applications they can trust are the ones treating HIPAA-guided practices as design inputs, not post-development verification steps.

Conclusion
Selecting a healthcare AI app development company is an architecture decision made in a procurement process. The vendor you choose will determine your data model, your AI model security posture, your EHR integration approach, and your HIPAA-guided technical safeguards. Those decisions will shape the application’s reliability, scalability, and clinical trustworthiness for years after launch. A vendor who understands that hospitals and enterprises have different architectural requirements, who conducts threat modeling before feature design, and who treats HIPAA-guided practices as foundational constraints rather than a compliance formality is making different, better decisions at every level of the engagement.
For hospitals and enterprises across California and the United States, the path to a healthcare AI application that delivers on its clinical promise starts with choosing the right development partner through the right evaluation process, before the first line of code commits you to an architecture you will live with for years.
Frequently Asked Questions
What is a healthcare AI app development company?
A healthcare AI app development company is a technology partner that designs, builds, and deploys AI-powered software applications for hospitals, health systems, payer organizations, and enterprise healthcare companies. These companies combine AI and machine learning engineering with deep knowledge of healthcare interoperability standards (HL7 FHIR), clinical workflow requirements, and the HIPAA-guided security architecture that healthcare applications require. The practical distinction between a genuine healthcare AI development company and a general software shop with healthcare clients is in how they approach architecture: security layer, EHR integration model, and data governance structure must be designed before application features, not alongside them.
What is the difference between healthcare AI app development for hospitals vs. enterprises?
Hospital AI development requires real-time clinical system integration, context-sensitive access controls mapped to specific clinical role relationships, and frequently on-premises or hybrid deployment to meet network isolation and latency requirements. Enterprise healthcare AI development requires multi-site data governance, site-specific AI model validation across different patient populations, API-first architecture for integration with enterprise platforms, and scalability designed for user volumes orders of magnitude larger than single-site hospital deployments. Development companies that use the same architecture template for both environments consistently produce applications that work for one entity type and fail operationally for the other.
How do HIPAA-guided practices shape the architecture of a healthcare AI application?
HIPAA-guided practices shape healthcare AI architecture across four technical safeguard categories defined in the Security Rule: access controls (unique user identification, context-calibrated session timeout, pre-built emergency access pathways), audit controls (append-only, cryptographically verified logging of every data access and model inference), integrity controls (immutable write-once records of AI-generated clinical content with model version attribution), and transmission security (TLS 1.3, certificate pinning for mobile, zero-trust service-to-service authentication). The integrity controls requirement is particularly significant for AI applications because the Security Rule was written before large language models existed: applying it correctly to AI-generated clinical content requires architectural decisions the original rule authors did not have to consider.
How do healthcare software vendors in the USA approach AI integration for hospital systems in California?
Healthcare software vendors serving California hospital systems must address both federal Security Rule requirements and California’s state-level data privacy regulations, which together create a more demanding data governance environment than most other U.S. markets. Hospital systems in San Diego, Los Angeles, and San Francisco are among the most active healthcare AI adopters in the country, and experienced vendors in these markets have developed specific expertise in FHIR-based EHR integrations, hybrid deployment models for hospitals with network isolation requirements, and multi-site data governance for California health systems that operate across diverse patient populations. The best California-focused healthcare AI vendors design state-specific data residency constraints and population variation considerations into their architecture before any features are scoped.
Is custom healthcare app development worth the investment compared to buying a packaged AI solution?
Custom healthcare app development is worth the investment when your organization’s clinical workflows, EHR environment, or patient population characteristics are not accurately served by available packaged platforms, which is true for most hospitals and enterprises operating beyond a standard single-site profile. Packaged AI solutions optimize for the median clinical use case and make architecture decisions you cannot override, including the data model, the access control approach, and the audit logging design. Custom development gives your organization full control over the security architecture, the EHR integration depth, the AI model validation methodology, and the site-specific calibration that production clinical AI requires.